Fractures
of the Femur
Fractures of the neck of the femur are common and are of two
types, subcapital and trochanteric. The subcapital fracture occurs in the
elderly and is usually produced by a minor trip or stumble. Subcapital femoral
neck fractures are particularly common in women after menopause. This gender
predisposition is because of a thinning of the cortical and trabecular bone
caused by estrogen deficiency. Avascular necrosis of the head is a common
complication. If the fragments are not impacted, considerable displacement
occurs. The strong muscles of the thigh, including the rectus femoris, the
adductor muscles, and the hamstring muscles, pull the distal fragment upward,
so that the leg is shortened (as measured from the anterior superior iliac
spine to the adductor tubercle or medial malleolus). The gluteus maximus, the
piriformis, the obturator internus, the gemelli, and the quadratus femoris
rotate the distal fragment laterally, as seen by the toes pointing laterally.

Trochanteric fractures commonly occur in the young and
middle aged as a result of direct trauma. The fracture line is extracapsular,
and both fragments have a profuse blood supply. If the bone fragments are not
impacted, the pull of the strong muscles will produce shortening and lateral
rotation of the leg, as previously explained.
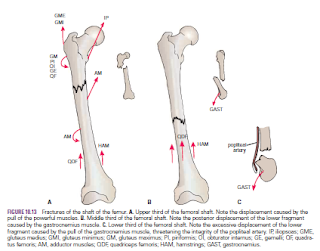
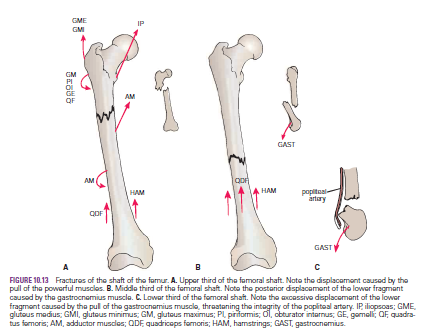
Fractures of the shaft of the femur usually occur in young
and healthy persons. In fractures of the upper third of the shaft of the femur,
the proximal fragment is flexed by the iliopsoas; abducted by the gluteus
medius and minimus; and laterally rotated by the gluteus maximus, the
piriformis, the obturator internus, the gemelli, and the quadratus femoris. The
lower fragment is adducted by the adductor muscles, pulled upward by the
hamstrings and quadriceps, and laterally rotated by the adductors and the
weight of the foot.
In fractures of the middle third of the shaft of the femur,
the distal fragment is pulled upward by the hamstrings and the quadriceps ,
resulting in considerable shortening. The distal fragment is also rotated
backward by the pull of the two heads of the gastrocnemius. In fractures of the
distal third of the shaft of the femur, the same displacement of the distal
fragment occurs as seen in fractures of the middle third of the shaft. However,
the distal fragment is smaller and is rotated backward by the gastrocnemius
muscle to a greater degree and may exert pressure on the popliteal artery and
interfere with the blood flow through the leg and foot.
From these accounts, it is clear that knowledge of the
different actions of the muscles of the leg is necessary to understand the
displacement of the fragments of a fractured femur.
Considerable traction on the distal fragment is usually
required to overcome the powerful muscles and restore the limb to its correct
length before manipulation and operative therapy to bring the proximal and
distal fragments into correct alignment