Humerus
The humerus articulates with the scapula at the shoulder
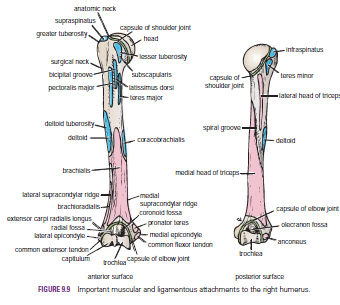
joint and with the radius and ulna at the elbow joint. The upper end of the
humerus has a head, which forms about one third of a sphere and articulates
with the glenoid cavity of the scapula. Immediately below the head is the
anatomic neck. Below the neck are the greater and lesser tuberosities,
separated from each other by the bicipital groove. Where the upper end of the
humerus joins the shaft is a narrow surgical neck. About halfway down the lateral
aspect of the shaft is a roughened elevation called the deltoid tuberosity.
Behind and below the tuberosity is a spiral groove, which accommodates the
radial nerve The lower end of the humerus possesses the medial and lateral
epicondyles for the attachment of muscles and ligaments, the rounded capitulum
for articulation with the head of the radius, and the pulley-shaped trochlea
for articulation with the trochlear notch of the ulna. Above the capitulum is
the radial fossa, which receives the head of the radius when the elbow is
flexed. Above the trochlea anteriorly is the coronoid fossa, which during the
same movement receives the coronoid process of the ulna. Above the trochlea
posteriorly is the olecranon fossa, which receives the olecranon process of the
ulna when the elbow joint is extended
Fractures
of the Proximal End of the Humerus
Humeral Head Fractures
Fractures of the humeral head can occur during the process
of anterior and posterior dislocations of the shoulder joint. The
fibrocartilaginous glenoid labrum of the scapula produces the fracture, and the
labrum can become jammed in the defect, making reduction of the shoulder joint
difficult
Greater Tuberosity Fractures
The greater tuberosity of the humerus can be fractured by
direct trauma, displaced by the glenoid labrum during dislocation of the shoulder
joint, or avulsed by violent contractions of the supraspinatus muscle. The bone
fragment will have the attachments of the supraspinatus, teres minor, and
infraspinatus muscles, whose tendons form part of the rotator cuff. When
associated with a shoulder dislocation, severe tearing of the cuff with the
fracture can result in the greater tuberosity remaining displaced posteriorly
after the shoulder joint has been reduced. In this situation, open reduction of
the fracture is necessary to attach the rotator cuff back into place.
Lesser Tuberosity Fractures
Occasionally, a lesser tuberosity fracture accompanies
posterior dislocation of the shoulder joint. The bone fragment receives the
insertion of the subscapularis tendon, a part of the rotator cuff.
Surgical Neck Fractures
The surgical neck of the humerus , which lies immediately distal
to the lesser tuberosity, can be fractured by a direct blow on the lateral aspect
of the shoulder or in an indirect manner by falling on the outstretched hand.
Fractures of the Shaft of the Humerus
Fractures of the humeral shaft are common; displacement of the
fragments depends on the relation of the site of fracture to the insertion of
the deltoid muscle. When the fracture line is proximal to the deltoid
insertion, the proximal fragment is adducted by the pectoralis major,
latissimus dorsi, and teres major muscles; the distal fragment is pulled
proximally by the deltoid, biceps, and triceps. When the fracture is distal to
the deltoid insertion, the proximal fragment is abducted by the deltoid, and
the distal fragment is pulled proximally by the biceps and triceps. The radial
nerve can be damaged where it lies in the spiral groove on the posterior
surface of the humerus under cover of the triceps muscle.
Fractures of the Distal End of the Humerus
Supracondylar fractures are common in children and occur
when the child falls on the outstretched hand with the elbow partially flexed.
Injuries to the median, radial, and ulnar nerves are not uncommon, although
function usually quickly returns after reduction of the fracture. Damage to or
pressure on the brachial artery can occur at the time of the fracture or from
swelling of the surrounding tissues; the circulation to the forearm may be
interfered with, leading to Volkmann’s ischemic contractureThe medial epicondyle (Fig. 9.10) can be avulsed by themedial collateral ligament of the elbow joint if the forearm
is forcibly abducted. The ulnar nerve can be injured at the
time of the fracture, can become involved later in the repair
process of the fracture (in the callus), or can undergo irritation
on the irregular bony surface after the bone fragments are
reunited
.

No comments:
Post a Comment